- Home
- All the way with Adam
- Analysing Trump-Turnbull Phone X-change
- Are we there yet ?
- Australia's diminishing political capital
- Boat turnback bribery and predictable silence
- Causes for Refugee Movements: Political Interference
- Corrupt Syndicate and Cover-ups
- Crimes of Secretary of DIBP (2011-2014)
- Details on Fazel Chgeni case:
- Election Season and Boat Secrecies
- Elephants and Lies -- Xmas season 2017
- End Offshore Slavery
- Evacuate the Asylum-seekers from Offshore Detention Centres
- Future for PNG Asylum-seekers
- Growing List of Hero Doctors
- Honesty is the best policy on payments to smugglers
- Lady Justice shines on the Pacific
- Lectures and Pressures
- Lets shine our solidarity on Manus Island and Nauru
- Lies, Spins, Cockroach and Rodents
- Ltr to Andrew Wilkie and Adam Brandt MP
- Media monopoly and conspiracy of silence
- Media monopoly: blackout vs spotlight
- Nauruan MOU and Dabwido -- Devil not in Him
- No Lecture, More Pressure
- OSB and Public Interest Immunity
- OSB, Turnbacks and Political cover-ups
- On wherever of the Internet
- Pacific Solution for Justice
- Refugees, Trust and Faith
- Royal Commission on Offshore Processing Regime, an initiative worth supporting
- Serving the Horizontal Outreach
- Shedding some light on OSB
- Should Dutton be sacked for adopting Cockroach Agenda
- Standing up for Refugees ? Set up a FB Group and Becomes Human Rights Information Retailer:
- The 2018 Unpacking of Xmas Lies
- The Syndicate of Corruption
- The myths, secrecies and refugee policy
- The scandal at hand
- Trade Your Vote for Refugees
- Treasonous minions
- UN Refugee Convention and Huston Report 2012 , a case of public mood-swings and government policy shift
- Virtual Communities - All about Respect
- Who gonna park on that spot ?
- Witchcraft behind the Spin
- Put yourself in Indonesian's shoes
- Australian Government's bribery payments to people smugglers
- Boat bribery payments and motives behind
- Labor, Liberal and Mandatory Detention Policy
- The Irony of Australian Government's "Tough on Crimes"
- Tilting at Canberra Windmills
- Why my polly is so silent
- The ALP Position on asylum-seekers detained offshore
- The Cowards of Australia
- Refugee Policy Moonwalks and ALP
- A Lie is a 'Lie' and a Crime is a 'Crime'
- Attributions
- AFP and ICC
- (2022-Sep) OTP-ICC Preliminary finding and Request for ICC jurisdiction
- (2018-Apr) Additional Submission to ICC re: Enslavement
- (2017-Jun) Enslavement in Manus Island and Nauru
- Dob-in to International Criminal Court
- Request ICRC to Evacuate Asylum-seekers
- Rome Statute Article 25 on Individual Responsiblity
- STATE OF TORTURE LAW IN AUSTRALIA
- Urgency on Offshore Situation
- Bomana
- Asylum Processing Under PNG/Naurual Laws: Lawful or Unlawful?
- Freedom Yours, Justice Ours
- LEGAL REMEDY FOR DETAINEES IN KP, MANTRA & ITAs
- ERRONEOUS OFFSHORE LAWS
- LIBERTY - BROADENING THE SCOPE
- EXECUTIVE EMERGENCY POWER, COMMON LAW AND ALIENS
- Bomana53# and Convention Obligation
- Legal Boundary of Offshore Processing Regime
- HCA Failed Offshore Detention Challenge S195/2016
- UNORG
- (Feb 2022) Submission to Human Rights Council and Special Rapporteur on Slavery
- (Sep-2019) Letter to UN Secretary-General Guterres
- (Sep-2018) Letter to President of Nauru and Prime Minister of New Zealand
- (Aug-2019) Resettlement Appeal to European Council
- (Jul-2019) Letter to Canadian PM Justin Trudeau
- (Dec-2017) Letter to President of ICRC
- Slavery
- Deaths in Detention
- Archived: 1992-2004
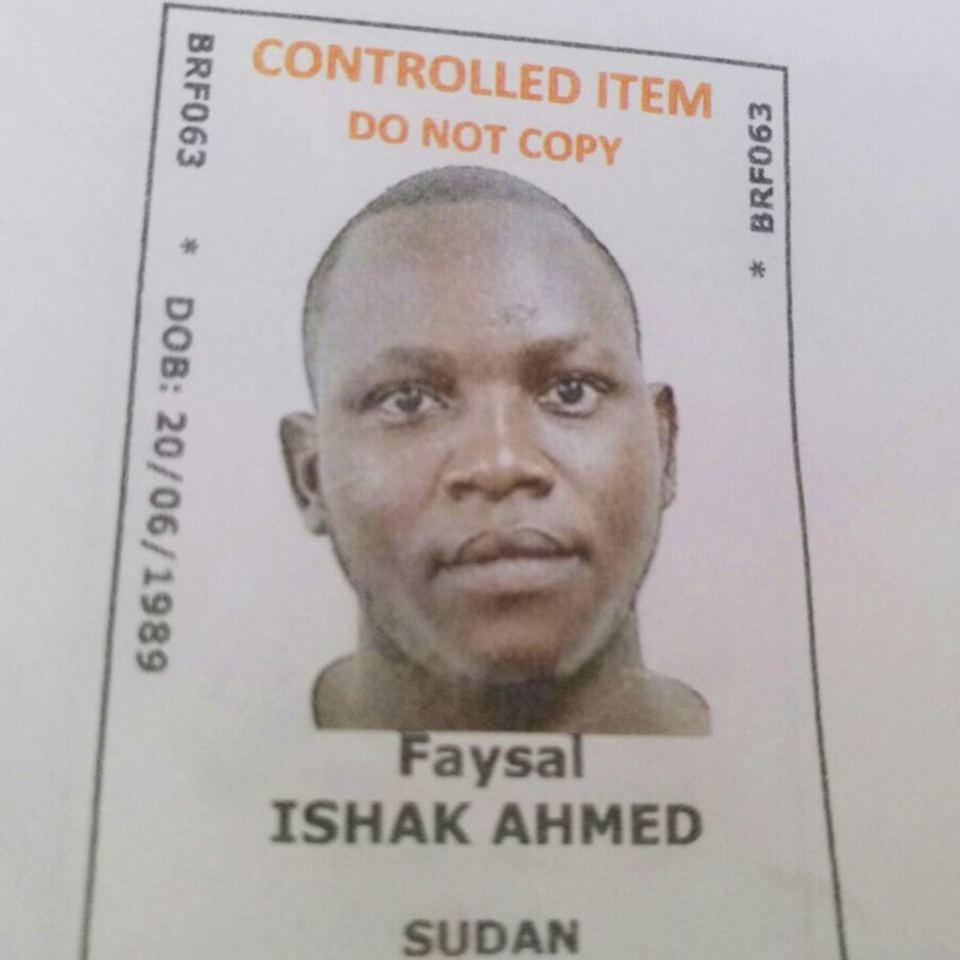
Faysal Ishak Ahmed (DOD 24-Dec-2016)
 Faysal Ahmed, Duty to Attend:
Faysal Ahmed, Duty to Attend: Faysal Ishak Ahmed:
Faysal Ishak Ahmed:;
 CONTENT GUIDE
CONTENT GUIDE
Created in 2019, this page features six colour-coded parts: Case Orientation, The Evidence, The Illness, The Laws and Crime, The Quest for Legal Action and also Other Writings.
N. Overview links of public media reports which describe the December 2016 incident of Sudanese refugee Faysal Ishak Ahmed (2016-2017)
I. The Evidence: Faysal Ishak Ahmed health incident (Oct 2021)
II. The Illness: Determination on type of illness and possible cause of death, based on evidence (Nov 2021)
III. The Laws and Crime: Application of slavery and torture laws upon specific health incidents (Dec 2021)
V. The Quest for Legal Actions: Despite authorities concealing material evidence, whether the public can now assert proper legal action against perpetrators (Aug 2022)
IV. Other Writings: Articles written since 2019 etc...
Faysal Ishak Ahmed,
Case Orientation
[Broadcast: 24 Jan 2023]
For those friends who're trying to familiarise the Manus Island medical evacuation delay on Faysal and the ABF/DIBP cover-ups, browsing into following lists of media reports would be very helpful.
First in-line would be this Sydney Morning Herald Article on 26/12/2016 by the journalist the (late) Michael Gordon. This article features one of the photographic evidentiary documents where Faysal stated, he visited the Manus Island clinic more than 20 times.
=> https://www.smh.com.au/national/dont-wait-treating-me--manus-detainee-fa...
The analysis on the nature & extent of ABF/DIBP cover-ups on illness/death of Faysal Ahmed had been given by the independent investigator, Kellie Tranter, on 15/5/2017, where she obtained FOI documents re: Faysal incident on December 2016. The ABF/DIBP ( or the Information Commissioner?? ) had redacted the spreadsheet that listed Faysal's clinic visitations and DIBP internal emails disputing the authenticity of the photographic evidence by SMH.
=> https://independentaustralia.net/life/life-display/pre-empting-faysal-ah...
The complete account on Faysal's background illness was documented by Behrouz Boochani on 30/12/2016 in the Guardian. According to Faysal's close friends (material witnesses), Faysal had been suffering from debilitating "stomach pain" over 2yrs period; where repeated blackouts had occurred in the last six months leading up to his final collapse in December 2016. It is possible that Faysal had a far more serious illness even before having symptoms of chest pain, muscle tightness and heart problems in the final six months. Remember, in law, such evidence is material in nature.
=> https://www.theguardian.com/commentisfree/2016/dec/30/faysal-ishak-ahmed...
On 10/2/2017, around Senate Inquiry, the Guardian's Ben Doherty again reported that Faysal had visited Manus Island clinics several times. Ben Doherty's writing is indicative of the journalists (SMH/Guardian) being aware of the existence of Faysal/IHMS correspondence (material evidence) from the very beginning, i.e. December 2016.
=> https://www.theguardian.com/commentisfree/2016/dec/30/faysal-ishak-ahmed...
The (late) Michael Gordon of 2016 SMH report on how Faysal/IHMS correspondences were obtained.
=> https://www.smh.com.au/politics/federal/i-need-you-guys-to-look-after-my...
I think this summed up well on the evidence & story. The copy of Faysal/IHMS correspondences, you can download from this link:
=> http://www.aus4iccwitness.org/evidence/20161231_faysal-ahmed-evidence.pdf
Faysal Ishak Ahmed, Case Orientation.
Quest for Public
Legal Actions Part-1
[Broadcast: 13 Aug 2022 (5-min R)]
FAYSAL AHMED, DUTY TO ATTEND AND PROXIMITY: Friends, in recent weeks we have the continuing discussion on the Australian common law about doctor-patient contractual relationships and corresponding doctor's legal duties that owing to his/her patient. This note, perhaps, is a bit of digression into the practical case of Faysal Ahmed, the Sudanese refugee who died in the Manus Island detention centre in December 2016.
In our discussion last year, I noted the lack of material evidence on the case of Faysal, especially for the general public, being summarised as:
=> (i) the result of the X-rays and blood tests, which Faysal Ishak Ahmed had undertaken par the instruction of IHMS-GP1 on 28/9/2016;
=>(ii) the diagnosis on those tests, which had already been disclosed to the Senate Committee on 11/2/2017;
=> (iii) the Coronial post-mortem results on the cause of death from Brisbane Hospital, which has now been sitting at the QLD Coroner's offices. The report result was said to have been completed after a year (2018).
The IHMS and DIBP to date have never officially recognised the illness symptoms that have been put forwards by Faysal himself -- heart problem, chest pain, muscle tightness etc. The Coroner in Brisbane had a preliminary inquest just before the last election. As a person in the general public, I am not privy to any of that information relating to those proceedings (NJP lawyers might have had some!). Although the last election had installed the new Labour government, we -- the public -- can be certain that in the ordinary course of events, the Coroner's report on the death of Faysal will be taken a few years more. In this respect, we shall continue to remain in the "information darkness", so to speak.
LACK OF MATERIAL EVIDENCE AGAINST PUBLIC ACTIONS
Without "officially recognised" material evidence, what kind of action can the public do to contribute towards Justice for Faysal; And all other Deaths and Offshore Slavery for that matter? The Coroner's Court, for a good reason, could not be pressed specifically to expedite its proceedings and urged to release any material to the public. In the meantime, the perpetrators of offshore slavery can sure be riding on merry-go-rounds and simply say "business as usual". Are we supposed to wait and see whilst the Commonwealth Government of any stripe may have been tactically delaying on that case? We, the general public, cannot know that !!
My friends, I am not simply here to curse the darkness but -- to the best of activist's tradition -- also to light up the candle! Since we the refugee activist community, of recent, have grown stout in legal understandings for offshore detention processes, we can be more assertive at commencing some public legal actions.
For a starter, I must recall two public petitions organised by Manus Island Sudanese Community (21/12/2016) and also the direct actions taken by Manus asylum-seekers concerning severely ill Faysal. Faysal Ahmed collapsed on 22/12/2016 in the camp and died on 24/12/2016 at Brisbane Hospital. In their petition on 21/12/2016 to IHMS, the Sudanese Community stated (see details [#%_101VE, [#3]]):
" ....advise .. person has got a real health problem and his condition is getting worse .... take it into consideration immediately before it is too late ...."
This petition, signed by Sudanese asylum-seekers on Manus, was in effect calling upon IHMS that Faysal Ishak Ahmed needed urgent medical attention; And also implying the situation was foreseeable that failure to give medical attention will result in catastrophic damages.
Again, on that day 21/12/2016, the asylum-seekers took Faysal Ahmed to detention centre gate, to see the doctor. The IHMS refused to see Faysal Ahmed ( see details [#%_100VE, [#3]]) .
"He had instability he could not sit in one place for just three minutes. He kept saying, "I cannot breathe. My heart is not working". And he was sweating a lot we (asylum-seekers) took him to the gate so as to see a doctor. But IHMS refused."
On the next day 22/12/2016, the asylum-seekers brought Faysal Ahmed to the cultural advisor and detention guards, advising them to take Faysal to IHMS. But the guards failed to do so.
".... We also advised them to take him to IHMS but did not listened to our advise. At 10:30am on Thursday, the 22nd of December 2016, he was taken to a room in the (VSRA) and they did not take him to a doctor. ...."
These documents appeared to have been widely distributed to the media and social media as of 31/12/2016.
IMPLICATIONS OF LAW
The failure by IHMS to see Faysal Ahmed in a medical emergency ( "failure to attend" ) and the failure by detention guards to bring Faysal Ahmed to the doctors ( "failure to render assistance" ) have violated laws. To my view, both incidents are legally actionable without requiring any of the other "material evidence" that listed in (i),(ii) or (iii) above. We can look at the NSW appeal case of "Lowns vs Woods (1996)" as a guide for "failure to attend" [#24].
In "Lowns vs Woods", in January 1987 Sydney, the 11-yrs old Patrick Woods had a severe epileptic seizure, known as grand mal seizure. His mother sent Patrick's 14-yrs old sister, Joanna to nearby clinics where Dr Peter Lowns had his practice. Dr Lowns had never seen Patrick before since Patrick Woods was not his regular nor registered patient. Therefore, the doctor rather advised Joanna to bring Patrick Woods to the clinics or otherwise refused. Despite the ambulance came, Patrick Woods had a prolonged seizure that ended up as quadriplegia. Dr Lowns was eventually liable for Patrick Woods damages. The court found Dr Lowns had "failure to attend" a medical emergency and ordered him to pay the sum of AUD $3.2 million as compensation.
One interesting point in common law is that there has been no "duty of care" for a person, or strictly speaking, medical practitioner to assist or intervene stranger who is in trouble. On quoting from [#24]:
"In general the common law does not impose a duty to assist a person in peril even where it is foreseeable that the consequence of a failure to assist will be the injury or death of the person imperilled. Something other than the foreseeability of harm is required before the law imposes a duty to intervene."
So then, what changed in the situation of Dr Lowns and Patrick Woods has been the action of 14-yrs old sister Joanna calling upon Dr Lowns for medical assistance. With that, certain legal duty then was created and imposed upon Dr Lowns to attend to the medical emergency. This is known in law as the principle of proximity, which creates a duty of care between two strangers.
LEGAL DOCTRINE OF PROXIMITY (NEXT)
We shall next look at the contents of "Lowns vs Woods", and see how we may apply these legal principles to the situation of Faysal. Perhaps, we can charted out a proper public legal action based on these knowledge. (TO BE CONTINUE..) -- NetIPR.
The Quest for Public Legal Actions: Part - 1
Quest for Public
Legal Actions Part-2
[Broadcast: 27 Aug 2022 (7-min R)]
FAYSAL AHMED AND DUTY OF CARE OWED BY COMMONWEALTH & ITS CONTRACTORS: Friends, in the previous note, we were looking at the NSW Appeal case of "Lowns vs Woods (1996)" [#24]; where the court held that the Sydney medical practitioner Dr Lowns had the duty to attend a patient in an emergency. The patient was 11-yrs old Patrick Woods, who at that time had been suffering from a severe epileptic seizure; but doctor Lowns and Patrick Woods never had any prior contact. The action of Patrick Woods's 14-yrs old sister, Joanna, in requesting urgent assistance from Dr Lowns said to have created the duty to attend. On breaching that duty, the Court ordered Dr Lowns to pay AUD 3.2 million for damages. Whilst the doctor and patient never had any other relationships, the court was using the principle of proximity to establish the doctor owed that duty.
On the case of Faysal Ahmed, for the efficacy of this discussion, I shall focus mainly on the duty owed to him by the detention contractors -- i.e. Broadspectrum, Wilson Security and IHMS -- within the context of the petition made by the Sudanese asylum-seekers community and also the direct actions taken by Manus Island detainees.
BY IHMS AND ITS DOCTORS
In contrast to the case of "Lowns v Woods", Faysal Ahmed had a pre-existing relationship with IHMS and its doctors. On this point, we do have evidence for such a relationship [#3]. In addition, the IHMS had been the sole contractor providing primary health care to the detainees. As such, the IHMS Organisation (Contractor IHMS) has contractual health care duty towards all detainees that has been stipulated by DIBP/IHMS contract. For the doctors deployed by IHMS Organisation, the duty of care exists towards Faysal Ahmed through the doctor-patient contract. The scope of a doctor's duty and obligation towards his/her patient was elucidated by CJ Brennan in "Breen vs Williams (HCA, 1996)" as [#23]:
"The provision of advice and treatment with reasonable skill and care may not exhaust the duty of the doctor. .... the doctor's obligation is to maintain or improve the health of the patient generally and to use reasonable skill and care in doing so, even though the advice or treatment .... is to be provided only on that occasion or for a limited time. The patient may be thought of as made of many parts some one of which may need treatment at a given time, but the patient is nonetheless an entirety whose life spans, or hopefully spans, the ills or disease of each moment. Once it is perceived that the duty of the doctor is owed to the patient as an entirety, it is not appropriate to assume that the duty is discharged merely by the giving of advice or treatment on the particular occasion."
As we have seen, a doctor's duty of care for the patient in the doctor-patient contract has not been limited only to the occasions of planned appointments for consultation, writing medical prescriptions or the patient getting out to the appropriate referrals. The terms of the contract extend to attending patients in the emergency as well. The latter duty for doctors is covered whether within or outside of the doctor-patient contract, as it arises in need of the patient at any point in time.
On point of laws, therefore, we have the existing relationship between Faysal Ishak Ahmed and IHMS Organisation; And also the evidence for the existing doctor-patient relationship between Faysal Ishak Ahmed and the doctors (GP1, GP2, GP3) who were deployed by IHMS on Manus Island. The Sudanese asylum-seeker community's petition and Manus Island detainees' direct actions, therefore, have established the fact upon which the IHMS and its doctors' duty to attend medical emergency for Faysal Ahmed. The IHMS and doctors breaching that duty to attend the medical emergency have attracted criminal liability. The intentional omission of duty has been established.
BY BROADSPECTRUM & WILSON SECURITY
As we all know, Faysal Ishak Ahmed and all Manus Island asylum-seekers until mid-2017, were in detention for the asylum-processing purpose by the Commonwealth Government. The contracting entities, BRS and Wilson Security were the detention authorities, who were acting as the agents of Commonwealth Government (DIBP). Obviously, for all legal purposes, the detention authorities have had a relationship with the detainee Faysal Ishak Ahmed. Also, the evidence is that the management of DIBP and BRS were aware that Faysal Ishak Ahmed had an unresolved illness. All employees of detention companies have the duty of care towards Manus Island detainees and Faysal Ishak Ahmed; about which the terms of the contract stipulated by DIBP/BROADSPECTRUM/WILSON SECURITY [ We need more details here; the public don't have direct access to those commercial contracts! ]. The BRS/Wilson Security and their employees are having the duty to assist detainees in distress and, especially, in a medical emergency. This has been a customarily accepted duty for detention companies, a fact that is not even required to invoke the legal principle of proximity. For example, in the 1985 HCA Judgment of "The Council of Shire of Sutherland v Heyman", the CJ Gibbs said [#22] :
"In deciding whether the necessary relationship exists, and the scope of the duty which it creates, it is necessary for the court to examine closely all the circumstances that throw light on the nature of the relationship between the parties. ........ If a relationship of neighbourhood or proximity is found to exist, then it will be necessary to proceed to the second stage of the inquiry. None of this process will be necessary if the facts fall into a category which has already been recognized by the authorities as attracting a duty of care, the scope of which is settled - e.g. no trial judge need inquire for himself whether one motorist on the highway owes a duty to another to avoid causing injury to the person or property of the latter, or what is the scope of that duty."
As regards the severely ill Faysal Ahmed, by the direct actions of Manus Island asylum-seekers, a proper and unambiguous request for assistance has been made to the detention guards of BRS/Wilson Security. The detention guards' failure to bring Faysal Ishak Ahmed to the medical doctors in an emergency breached the duty to assist, and that has attracted criminal liability. The intentional omission of duty has been established.
THE REACH OF TORTURE AND SLAVERY LAWS
As has been outlined in "Sec X. Medevac & Common Law .. in Offshore Detention.... " [#9], the direction I have taken here is, firstly, to establish criminal liability in the authorities' omission of duty as the breach of torture law. The standard two-pronged test for detecting the existence of torture concerning the medical care of the incarcerated are: (1) there must be proof of a serious medical need of the detainee/prisoner (2) the acts or omissions by detention officials that indicate deliberate indifference to that need [#25].
For proof of Faysal Ishak Ahmed was so obviously in serious medical needs, the court can take direct eye-witness evidence from Manus Island asylum-seekers. The "serious" medical need of a person (prisoner) may be regarded as one that has been EITHER "diagnosed by a physician as requiring treatment" OR one that is "so obvious" that a lay person would easily recognize the necessity for a doctor's attention [#16].
Do note here: Because of the strength of evidence from petitions ([#%_101VE, [#3]]) and direct actions ([#%_100VE, [#3]]) by those of Sudanese & Manus Island asylum-seeker communities, one could now bypass officially recognized information on (i),(ii) & (iii) for material evidence. The general public and Manus Island asylum-seekers can now supply direct material evidence for proper legal action, entirely independent of those official sources.
As we are well aware, under the Australian Criminal Code Act 1995(Cth), both Torture law (Div. 274) and Slavery law (Div. 270), and also these laws under ICC provisions, that are applicable with "s 15.4 extended geographical jurisdictions -- category D". As such, the criminal violations that had taken place at offshore processing centres on Manus Island and Nauru are within the jurisdiction of Australian domestic courts.
Friends, I am therefore of the view that all the requisite laws along with substantive material evidence have now been in place. It is a matter of we -- the public and Manus/Nauru asylum-seekers -- gathering amongst ourselves and properly putting these things before the trier of fact.
THE UTILITY OF PROXIMITY PRINCIPLE
The entire event of the failure to medically evacuate Faysal Ahmed can be characterised as an act of torture. Presently considered two instances of refusal by detention authorities are parts of the act of torture. By comparing with the case of "Lowns v Woods" within the principle of proximity, we can see the omission of duty on Faysal Ahmed had gone beyond what can be termed as the usual medical negligence. It is the authorities' failure to observe their humanitarian obligations. It is the inhuman conduct that calls for proper legal redress.
Friends, I will now getting back to the main discussion on doctor-patient relationship on [#9]. Keep informed with updates and actions on that URL. -- Cheers, NetIPR.
The Quest for Public Legal Actions: Part - 2
Personal Criminal Liabilities
for IHMS and Its Personnel
[Broadcast: 19th Dec 2021 (7-min R)]
Friends, since early November 2021, we have started analysing the possible violations of Torture and Slavery laws by Commonwealth Government and its offshore detention contractors, with a case by case basis on Samuel (anonymous) [#6] and Faysal Ishak Ahmed [#15]. These detailed analytical considerations on a case-by-case basis have to be understood also as part of the larger project on the determination of the Crime Against Humanity of Enslavement [#9], of which we started the discussion in Feb/Mar-2021. We've observed that, because of the intervention and obstruction made by DIBP/ABF in the healthcare sector, the primary health services rendered by IHMS and its GP doctors to asylum-seekers became ineffectual. Because of the DIBP interventions, IHMS and its GPs in particular were contractually bound not to independently provide healthcare services to asylum-seekers in offshore detention settings. Seeing this in human rights contexts, such DIBP's conduct is tantamount to extinguishing an asylum-seekers' inalienable right to manage one's own health. Consequently, the asylum-seekers who became ill and needed higher-level care were confined to the detention camp. Such government and detention contractors violating the human rights of asylum-seekers are seen in the Torture and Slavery laws as:
=> When an asylum-seeker has been `denied` or `deliberately rendered ineffectual` medical treatment, the Commonwealth Government, the IHMS and its GPs have violated the law of torture;
=> When such medical intervention by DIBP/ABF has restricted the freedom of movement for that asylum-seeker, the corresponding DIBP/ABF conduct has violated slavery laws. The IHMS and its GP may also found to be violating slavery laws.
We have seen in our example cases of Samuel and Faysal, how the violations of these laws have taken place. I'll now move on to determining the specific conduct of the "possibly" three IHMS-GPs, who refused to disclose to Faysal in regards to his personal health information on which what kind of illness Faysal may have been suffering from. Upon reviewing hand-written notes by Faysal and the community witness statements (100VE, 101VE of [#3]), it is clear that Faysal had been repeatedly asking the IHMS-GPs about his illness, in particular, that causing his chest pain and heart problems.
CONTENTS: LAWS AND CRIME
- In this 3-parts discussion on laws and crime, the conduct of DIBP, IHMS and their personnel towards Faysal Ahmed had been projected onto violation of slavery and torture laws.
- Part-1 observes that the type of illness Faysal Ahmed suffered is consistent with cardiogenic pulmonary edema. Such type of chronic heart failure could not have developed overnight. It's therefore concluded the IHMS and DIBP were aware of Faysal's illness long before September to December 2016.
- Part-3 examines the nature of political control that Commonwealth (DIBP) had exercised over offshore processing centres that directly impacted upon the illness of Faysal Ahmed. It observes the control extinguishes the inalienable rights to the health of asylum-seekers under detention.
- In addition, such political control exercised over Faysal Ahmed had wiped out any chance for Faysal Ahmed to seek any other help and support he needed for managing his ailments.
- Seen within the context of political control, the roles taken by IHMS and its personnel were each found to have personal criminal liability. Such liability heavily weighs upon IHMS-GPs who traditionally have the role and responsibility of entrusted persons.
- Faysal Ahmed was 'categorically denied' the treatment for his chest pains and breathing problems. In several instances, the IHMS had rendered 'ineffectual treatment' for Faysal. Consequent violations of laws have been discussed in Part-2.
- The IHMS-GPs' refusal to provide personal health information to Faysal Ahmed prevented him from seeking further help. The consequent violation of laws has been discussed in Part-3.
Faysal Ahmed, of course, would have been the person in a state of severely unwell, especially from onward September to December 2016. By late September 2016, we know that he had undertaken chest X-rays and blood tests. Again, with those test results, along with accumulated health data from Faysal's earlier visits, any reasonably trained medical doctor, or even experienced nurses, would have been able to provide some preliminary diagnosis or to conclude the decision on further referral. [As a layperson, my projection for Faysal illness has been "pulmonary edema", which I've based on publicly available health information.] In any case, it is unfathomable for a GP of any stripe and colour may try to withhold personal health information from a patient in the face of severely deteriorating health as is in the case of Faysal.
STATE OF MIND AND PERSONAL CRIMINAL LIABILITY
Powerful laws as they are, both Torture and Slavery laws have set themselves apart from other classes of crimes when it comes to criminal intent. For instance, in ordinary crimes of battery or murder, the prosecution has to prove that the accused person indeed had the criminal intent or criminal state of mind (mens reas, fault element (AUS)) when he/she was committing the actual act of crime (actus reus, physical element (AUS)). Slavery law has `strict` liability and Torture law has `absolute` liability. The crimes with these types of liabilities, the prosecution is not required to prove the accused person has had proper criminal intent or criminal state of mind (mens reas) when he/she was committing the crime. However, it is instructive to eliminate any additional factors such as any duress that could have been imposed upon those GPs.
POLITICAL CONTROL AGAINST FAYSAL ILLNESS
The DIBP/ABF decision to intervene in Faysal's medical treatment, undoubtedly, had been based on political considerations. We know that during 2014-2016 in the aftermath of the violent death of Reza Barati, the Australian public as well as activists around the world were focusing on Manus Island detention centre. Within the camp also, there was constant strife (hunger strikes, protests etc) staged up by refugees to break the deadlock. The LNP Government with detention groups had countered these social movements with the mass media campaign of dehumanising refugees. On the official front, the emphasis has been made till today that asylum-seekers offshore are not Australia's responsibility and that they are the 'matters for PNG/Nauruan governments'. The primary objective of LNP Government was to keep total political control of the offshore detention situation around that time.
Within this environment, any piece of information or a concrete indication that the Manus Island refugee Faysal has been requiring medical care could have turned things around. Potentially, it is untenable for the LNP Government to 'knowingly' keep an asylum-seeker on Manus Island who has been severely ill with possible heart conditions were to have been left untreated. The refugee-supporting lawyer groups in such cases might try a court injunction to bring Faysal to Australia, which will threaten the offshore detention regime. A case of the sick refugee on Manus Island could also become the trigger for compassion-based and right-based community groups to rally against offshore detention. In politics, anything could be possible.
In all probability, therefore, the DIBP/ABF seemed to have kept everything silent on Faysal's need for higher-level medical care; including a total prohibition on disclosing the doctor's diagnosis information for Faysal's chest pain and heart problems.
OWNERSHIP OF PERSONAL HEALTH INFORMATION
The Australian Medical Association Ethical Guideline [#8] required the treating doctor to appropriately disclose to the patient in regards to his/her illness and must also explain possible treatment plans (rule (g_)). A patient obviously may not understand his/her illness in full medical terms. However, the treating doctor must explain in layman's language about the patient's illness. The IHMS organisation and its GPs withholding personal health information from Faysal, therefore, are against this guideline.
In principle, any information a person has produced would belong to that person. Say, for example, when I go to a supermarket, buying products X,Y and Z, it will be my personal information. I have a phone and when I call the numbers A, B and C, it would also be my personal information. Typically, I am the primary owner of that personal information and the supermarket and phone company -- although they in part contributed to producing such information -- are not allowed to transfer, disclose or sell out my personal information.
It is, therefore, Faysal Ahmed who is the primary owner of his personal health information. The IHMS organisation and its GPs, although have contributed to producing Faysal's personal health information, they are not entitled to be held in possession of Faysal's personal health information. Customarily, healthcare providers and GPs are required to disclose personal health information when the patient has requested it.
EXERCISE OF POSSESSION IN CHATTEL SLAVE ANALOGY
As explained above, a person's health-related information primarily will belong to that person. This also is true for work and labour: A worker's fruits of labour, in form of monetary gains or product outcomes, typically belong to that worker. A family's offspring which the parents produced, i.e. sons and daughters, the parents cannot exactly own but the children do belong to their parents.
In a classic chattel scenario, a slave owner would claim ownership of everything the slave had produced -- the fruits of labour including the slave's offspring children.
Healthcare Providers and GPs are reasonably expected to provide appropriate personal health information when the patient has made the request. The IHMS organisation and its GPs which claimed possession and withholding as their own of personal health information that rightfully belongs to Faysal Ishak Ahmed is slavery. In other words, the conduct of IHMS and its GPs tantamount to exercising one of the powers attached to the rights of ownership, namely the right to possess, not exactly over the person of Faysal Ahmed himself, but over the health-related information that is rightful belongings of Faysal Ahmed. To my view, these slavery charges on IHMS and its GPs would withstand even in the absence of any DIBP/ABF directives.
In addition, by withholding the critical health information from Faysal, the IHMS organisation and its GPs had directly contributed to the DIBP/ABF objective of keeping Faysal in Manus Island detention centre. Therefore, on the account of withholding information, along with DIBP/ABF, the IHMS organisation and its GPs have co-perpetrated in exercising one of the powers attached to the rights of ownership, namely the right to security, over Faysal Ishak Ahmed.
WHAT IS THE STATE OF MIND ?
The inhuman conduct of IHMS personnel on Manus Islands towards Faysal Ahmed has now been clear: refusing and failing to assist the patient who's having a life-threatening illness. One would wonder what has propelled those IHMS personnel to commit a such heinous crime? The comparison wouldn't fit the WW-II SS Nazi doctor Fritz Klein of Auchwitz [#18], who possibly had administered the death gas over several thousand Jewish prisoners: He was a rabid racist. But IHMS-GPs and personnel aren't such kinds of racists, I am pretty sure.
For those IHMS-GPs, having to observe the terms of the contract won't be providing a defence for committing any crime. There are no other compelling reasons to be found in participating in the crime. They are civilian contractors and, as such, they are free at their will to fly out of Manus Island, if they decide not to be part of the crime. It is therefore we are to conclude that the "criminal opportunism" of these IHMS-GPs a possible state of mind. Simply states: they have committed these crimes because they believed they can get away with it!
Friends, with this note, I shall wind up discussion on the case of Faysal. Please keep yourselves updated with the website (www.aus4iccwitness.org) throughout this X-mas period.
-- Regards, NetIPR.
The Laws & Crime: Part - 3
Untenable Position of
IHMS-GPs
[Broadcast: 5th Dec 2021 (6-min R)]
Friends, week by week, as we have progressed our discussion onto individual enslavement cases for Faysal Ahmed and Samuel, we sure are gaining our grips on understanding about the way Commonwealth Government exercising the power of control over the medical movement of offshore asylum-seekers. We've already observed that the three levels on which the government and detention groups may have violated laws as they exerted control over asylum-seekers' medical transfer and related healthcare issues:
(iii) The DIBP/ABF (Commonwealth Government) will be found, at governmental policy and on nation-state level, to have violated the slavery and torture laws;
(ii) The IHMS will be found, at the contractually bounded organisation level, to have violated the slavery and torture laws;
(i) The clinicians (GPs and Nurses) who have had direct contact with asylum-seekers may be found, at the personal level, by themselves or as the agent of IHMS, to have violated slavery and torture laws. That has been demonstrated in the case of Faysal Ishak Ahmed.
CATEGORICAL DENIAL ON THE TYPE OF ILLNESS
We've briefly discussed in Section IX of [#9] that, the policy-level denial to treat a certain type of illness -- such as psychiatrist-related illness -- will be found to have violated the torture laws. For detailed consideration, we can draw an analogy from the cases in the United States that [#2]:
"categorical denial of [elective, nontherapeutic abortions] constitutes deliberate indifference to serious medical needs under [both prongs of Estelle]."
I'd put in square brackets to emphasize that, say for example, the policy to provide "no treatment" to any non-life threatening illnesses, despite recommendations made by a psychiatrist or even by a lay person, can constitute a violation of torture laws. We've already observed this particular evidence in PE_002 & PE_003 of [#7], where the government's policy-level violation of torture laws had taken place.
CATEGORICAL DENIAL TO TREAT THE ILLNESS OF FAYSAL AHMED
The IHMS-GPs (1, 2 & 3) refused to look into and categorically denying to give the treatment for Faysal's illness symptoms of "chest pains and heart condition" have constituted torture. The violation of slavery laws would automatically be followed. This categorical denial of illness symptoms of Faysal was not instituted at the DIBP/ABF policy level. However, we can assume such instruction to deny higher level care must have to come down from DIBP/ABF as a direct intervention that effecting individual patient Faysal. The involvement of IHMS at the organisational level may be clear from the fact that all GPs had refused to look into Faysal's main complaint about chest pains and heart conditions (see 100_VE & 101_VE of [#3]).
We've got to be aware that Faysal was, just like the rest of us, a "lay person" in terms of medical knowledge. However, Fayasl, the layperson, could not have been mistaken about the chest pains he suffered and the irregular heart conditions that he had had. Therefore:
=> "Holding a serious medical need is `one that has been diagnosed by a physician as requiring treatment or one that is so obvious that a lay person would easily recognize the necessity for a doctor's attention`"[#2]
As a general rule, it is not required that a latent health issues -- such as heart problems and chest pains -- blossoming into full fledged health crisis before these symptoms are being considered as serious [#13]. Faysal Ahmed had presented these symptoms to IHMS doctors earlier than September 2016. Faysal's medical needs became evidently serious in the period of Sept-Dec 2016 due to the IHMS doctors denial :
=> "Finding medical needs may be deemed serious if the denial or delay potentially would result in serious injury, long term harm, or permanent disability"[#2]
To our observations, the most likely cause of death for Faysal Ahmed been "pulmonary edema", which is the consequence of chronic (long-term) heart failures (See "Cause of Death" [#15]). The dispute that took place between Faysal and IHMS-GPs is not a mere disagreement about what may constitute proper medical treatment. The evidence is that the IHMS Organisation and those GPs it deployed on Manus Island had shown deliberate indifference to the serious medical needs of Faysal Ahmed.
By categorically denying to give treatment for the symptoms of chest pain and heart problems presented by Faysal Ahmed, the personnel and organisation of IHMS, therefore, had violated the torture law.
In so denying medical treatment to Faysal Ahmed, the DIBP/ABF and IHMS have also committed the crime of confining Faysal to Manus Island detention centre. This is the exercise of one of the powers attaching to the right of ownership, namely the right to security, over Faysal Ishak Ahmed. This constituted a violation of slavery laws by DIBP/ABF and IHMS.
RENDERING INEFFECTUAL TREATMENT
On looking through the detailed narrative provided by 100_VE [#3], the IHMS GPs put on Faysal certain medication for three months, which Faysal find no improvement in his illness condition. We, ordinary folks or even experienced doctors, could not make a second guess as to what the treating doctor might be doing to his/her patient. However, this has been such an exceptional circumstance that the IHMS doctor might have been prescribing some medication to Faysal to reduce fluid in the lungs; or the doctor may try to treat possible infections that can cause pulmonary edema [#12]. It became evident by Sept-Dec 2016 that treatments undertaken by Faysal had had no impact and that a specialist examination with higher-level care have been required for Faysal.
For pulmonary edema and underlying health problems, the risks of inadequate treatment were obvious to a reasonably well-trained doctor, nurse or medical officers and the IHMS Personnel were subjectively aware of the risks. But they did not respond reasonably. Such conduct constitutes exhibiting deliberate indifference to the serious medical needs of Faysal.
Deliberate indifference also occurs when the doctor continues a type of treatment known to be ineffective and administered in the face of resultant pain and risk of permanent injury [#16].
Therefore, by rendering and persisting on ineffectual treatment to Faysal, the personnel and organisation of IHMS have exhibited deliberate indifference to the serious medical needs of Faysal. They have done so such conduct under instructions of DIBP/ABF, which constituted a violation of torture laws. Slavery laws violation is the same as above.
UNTENABLE POSITION OF IHMS-GPs
The Senior Medical Officer and Health Service Managers deployed by IHMS at Manus Island were former senior nurses [#1]. As such, all clinicians who have direct contact with Faysal are well aware of AMA Code of Ethics. We know that any clinicians, particularly doctors, breaking such Code of Ethics will become violating various laws. As we delve deeper into the detailed conduct of DIBP/ABF and IHMS, we're reaching an inevitable conclusion as to the untenable positions of the IHMS doctors that can be equated to criminals who have no respect for the "right to health" and "right to life" of human persons. Such sentiment was already reflected by Dr. Peter Young [#17]:
"The appropriate medical response is to advocate to stop the cause of suffering rather than to continue to apply less and less effective band aid responses while propping up a damaging system and providing convenient cover for the government. Within the system no advocacy is allowed, stating medical facts or giving clinical opinions which counter department aims is considered political and leads to swift sanctions."
"It is extremely difficult for doctors, nurses, psychologists and other health workers to acknowledge that sometimes being involved in a system does more harm than good. Proposals to boycott have been controversial but in my view, it is the government that has decided to impose conditions that do not allow normal practice to occur, and health professionals should not practice where these standards are not met."[#17]
The Laws & Crime: Part - 2
Ethical Rules and
Command Responsibility
[Broadcast: 21st Nov 2021 (7-min R)]
In the last week's posting, we observed the possibility that Faysal had suffered from some form of "heart failure", where the consequent cause of death been identified "pulmonary edema", which is a type of illness that can gradually get worsened in people. The kind of illness Faysal had can be contrasted with the sepsis infections suffered by Hamid Khazaei, an illness that can develop into a deadly condition in a matter of days. Therefore, given the number of visits Faysal made to the Manus Island clinics, we can conclude that IHMS Personnel and DIBP/ABF were aware of his illness situation well before September 2016.
DETENTION ENVIRONMENT
The asylum-seekers on Manus Island in the period of July 2013 to October 2017 were being held under proper detention. They were confined to the campsite and watched over by the security guards. No independent NGOs were allowed in the camp. Communication with the outside world in the form of internet messages and phone calls has been allowed. But those asylum-seekers who were lacking personal communication skills, i.e. English language and the use of technology, would have been completely isolated. We've got to remember that one of the primary objectives of the Commonwealth Government for establishing offshore detention has been to isolate detainees from refugee support groups to deprive asylum-seekers accessing lawyers and courts in Australia.
Within the DIBP, the written order to resist overseas Request for Medical Movement (RMM) was already in place since June 2015, directing only to transfer a person in a life or death situation [PE_003, #7]. As of 29 April 2016, Secretary Pezzullo again reiterated this position (See. PE_003, [#7]):
Secretary Directive stating 'the aim should be to avoid to the maximum extent possible such transference to Australia ... This instruction is to be overridden only if and when there is a reasonable apprehension that inaction would result in an immediate threat to life, or the occasioning of permanent debilitating injury'..
These are the Ministerial level orders of which "as strictly as possible" implementations required by the contractor IHMS, and the civil servants within DIBP/ABF. Under this environment, any RMMs put forward by IHMS for Faysal would have been refused.
We've got to be aware that the PE_003 [#7] is the evidence for the occurrence of state-sanctioned torture, stemming from the governmental policy, that exhibits deliberate indifference to the serious medical needs of a person who has been under the custody of the Commonwealth.
UNETHICAL CONDUCT, CRIMINAL CULPABILITY AND COMMAND RESPONSIBILITY
Let us first focus on the ethical responsibility of the IHMS-GPs towards Faysal, who is their patient in the detention setting. Although these GPs were all contracted out to and paid for by the IHMS, when treating the illness of Faysal Ishak Ahmed, they must discharge their healthcare duties to Faysal as independent doctors. Here the notion of "discharging healthcare duties as an independent doctor" has been of primary importance. Let's say, when I am visiting a GP in my local area of Sydney, that GP is required to give me his health advice and assessment as an independent doctor to the best of his knowledge and expertise without being influenced by any other factors. The same ethical standards must be applied to the IHMS-GPs who had been working under and paid for by IHMS & DIBP/ABF in treating the illness of Faysal Ishak Ahmed, the asylum-seeker in detention.
In Section VII of [#9], we've discussed the ethical rules (a_ to j_) for doctors when treating a patient. Of course, the above listing of rules (a_ to j_) may reflect core ethical values but they cannot be exhaustive in practical terms, simply because of the complex legal, social and cultural factors that needed to be taken into account when a doctor interacting with a patient. By cross-checking the Australian Medical Association Code of Ethics [#8], a treating clinicians must observe these rules:
(a_) treat all patients without discrimination;
(b_) patient's well-being is the first priority;
(c_) patient must be allowed to manage his/her own health;
(d_) patient has the right to choose; and right to change doctor & treatment;
(e_) patient has the right to withdraw from treatment;
(f_) informed consent must be given on every stage of the treatment;
(g_) the patient must be informed about his/her illness and explained about possible treatment plans;
(h_) The guardian of a child must manage the health of the child under his/her care
(j_) the treating doctor must have the autonomy;
As discussed in Section VII of [#9], when a treating clinician break those ethical rules, that will violate inalienable right to health of the patient. As a result, that treating doctor (clinician) will found to be violating various laws.
The IHMS-GPs on Manus Island, in first look, have violated ethical rules (g_) and (b_) when treating Faysal. When IHMS-GPs refused to provide Faysal with X-ray and blood test results, which he had undertaken after 28/9/2016, violate the ethical rule (g_). That conduct by IHMS-GP in withholding critical personal health information from Faysal also violated slavery laws.
When IHMS-GPs -- the GP2 & GP3 conducts on public evidence -- failed to immediately send severely ill Faysal to the hospital to receive higher care, these GPs violate the ethical rule (b_). The conduct of these IHMS-GPs' omission to send severely ill Faysal to the hospital has violated both slavery and torture laws.
Predictably, the conduct of these IHMS-GPs will have criminal culpability for themselves, and the effect will link up in the commands on IHMS and ABF/DIBP. For example, when the IHMS GP (1,2 &3) failed to send severely ill Faysal to the hospital, that GP obviously had not acted in the "best interest" of the patient Faysal (b_). That GP's conduct will be construed as the contractor of IHMS, who also is an agent of DIBP/ABF, exercising the right to security over Faysal. This is a violation of slavery law. Again, by failing to send the severely ill Faysal to the hospital, the GP exhibited deliberate indifference to the serious medical needs of Faysal. Therefore, the GP personally and as the agent/contractor had violated torture laws.
If this GP were to provide a defence at the court -- surely he/she would -- that he/she had done so the violation (b_) under the superior orders of IHMS and his/her contractual obligations, it will be evidence that he/she has had no autonomy treating patients (j_). When the GP has no autonomy in making an independent decision on Faysal's illness, we can conclude that his/her superiors (DIBP/ABF and IHMS) have exercised one of the powers attaching to the right of ownership, namely the right to manage, over Faysal.
Within the above analysis, we can predict that the personnel and organisations of IHMS and DIBP/ABF will be found violating slavery and torture laws at various levels.
(i) The clinicians (GPs and Nurses) who have had direct contact with Faysal will be found, at the personal level, by themselves or as the agent of IHMS, to have violated slavery and torture laws;
(ii) The IHMS will be found, at the contractually bounded organisation level, to have violated the slavery and torture laws on the case of Faysal. The superior responsibility needs to be followed.
(iii) The DIBP/ABF (Commonwealth Government) will be found, at governmental policy and on the nation-state level, to have violated the slavery and torture laws in the case of Faysal. Superior responsibility consideration should have to be followed.
Remember also that, in addition to the slavery and torture laws under Australian jurisdiction, those IHMS-GPs who had violated the rule (b_) against Faysal will have culpability under various criminal laws within the jurisdiction of PNG, such as conducts that intentionally caused the person of injury, pain and eventual death. This, of course, is outside the scope of the current discussion.
CALCULATED RISK TAKINGS
My observation is that the architects of Australia's offshore detention regime may have foreseen the possibility of criminal violations within the jurisdiction of PNG, as just outlined in the above paragraph. But those architects -- probably quite rightly -- predicted that the refugee supporters would have no resources to legally challenge within the jurisdictions of PNG and Nauru in such cases as Faysal Ahmed.
Successive LNP Governments with those "behind the scene" architects, traditionally have given no regard to international human rights laws [#10]. Exploiting the lack of enforcement in these international laws areas, the government have given scant attention to the instances of "detention" and "non-refoulement". These offshore architects might have, at one time, been thinking over the international torture laws (See AE_009, evidence). But, the DIBP (Commonwealth) main defence was solely based on the MOUs it had signed with PNG and Nauruan governments. It appears that the architects are completely oblivious to the Australian Torture and Slavery laws that have extended geographical jurisdictions. Of course, not knowing the laws cannot be a legitimate defence for committing the crime.
The Laws & Crime: Part - 1
The Illness of
Faysal Ishak Ahmed
[Broadcast: 14th Nov 2021 (4-min R)]
Friends, in previous posting "Timeline On Faysal Ahmed Health Incident" , I've drawn similarity of circumstances between the case of Samuel [#6] and the treatment period of IHMS-GP1 with Faysal. Based on the nature of the evidence we have had, I shall further be dividing up the crime counts that should be applied to all IHMS GPs; and the counts that can be applied only to IHMS GP2 and GP3. This, in part, is to demonstrate the point that the Commonwealth Government and detention groups withholding certain material evidence on the case of Faysal will have no protective effect regarding the application of the slavery and torture laws.
CONTENTS: THE ILLNESS
- This section examines the details of the illness of Faysal Ahmed and then postulated the type of illness he may have suffered and also the possible cause of death.
- Determining the type of illness based on publicly available information is to serve the discerning public. This measure is also to fill the void of authorities failing to provide any information regarding the illness of Faysal Ahmed. The laws and the court, in principle, would not require to serve the correct diagnosis of illness of the deceased person. Suffice only providing the factual evidence of Faysal Ahmed had been suffering from a serious illness.
- The illness and sufferings of Faysal Ahmed had been eye-witnessed by the asylum-seeker inmates till its final days. One of the witnesses, a cartoon artist, who was with Faysal Ahmed had documented the last hours before the eventual collapse of Faysal on 22nd December 2016.
- Deriving from the evidence disclosed as of December 2021, Faysal Ahmed may have been suffering from long-term cardiogenic pulmonary edema. Faysal died either from pulmonary edema (40%) or pleural effusion (60%). Heart failure is to be a primary underlying cause for the build-up of excess fluid in Faysal's lungs.
- As of January 2023, publicly disclosed evidence indicating that Faysal Ahmed may have an underlying serious illness that developed into pleural effusion.
THE CRIME OF DIBP/ABF AND IHMS AT FIRST GLANCE
On 8/2/2017, during the Senate Inquiry on offshore detention, West Australian Senator Pat Dodson raised concerns with DIBP about the death of Faysal Ahmed [#1]:
"... That is a bit difficult when you are seeing an individual turning up 20 times to a clinic and no-one has come to a view that there is something seriously wrong with that individual. That seems to be the case with (Faysal) Ahmed...."
The IHMS diagnosis for Faysal was given in a closed session of inquiry by Dr Brayley of ABF later that evening. The coronial report on the death of Faysal sits with Queensland Coroner's Court since 2018. For slavery and torture laws, the correct medical diagnosis for illness of Faysal doesn't need to be served as evidence. This simply is because when detention authorities denied reasonable requests for medical treatment.. and such denial exposes the inmate "to undue suffering or ... injury", the deliberate indifference is already in manifest [#2].
Again, the seriousness of an inmate's medical need may also be determined by reference to the effect of denying the particular treatment. Also, the denial or delay causes an inmate to suffer a life-long handicap or permanent loss, the medical need is considered serious [#2]. It is self-evident (i) Faysal had a serious illness that caused eventual death and (ii) the IHMS had denied him the requested medical treatment. This would have formed, in my view, enough grounds to proceed with charges against DIBP/ABF and IHMS.
Nevertheless, the detailed accounts of what had happened to Faysal have been important for the satisfaction of the discerning public. Therefore, we must reconstruct the events that surround the death of Faysal as practically as possible. Since a proper report by Coroner could be years away, and the Commonwealth authorities are sure to withhold any incriminating information as long as possible, I am making sure I filled the gaps for missing parts of events in a commonsense manner based on publicly available information. As you would all see, our knowledge gained in the case of Samuel has greatly assisted us in evaluating the internal procedures of IHMS and DIBP/ABF.
WHAT KIND OF ILLNESS FAYSAL MAY HAVE SUFFERED ?
The symptoms of illness described repeatedly by Faysal himself are "heart problems, muscle tightness, chest pains and difficulty in breathing [100VE, #3]". From the linked Cardio information site, Faysal may have been suffering from a certain form of "heart failure" [#4, #5]. The situation of Faysal in the week before his death had been reported as "...He had instability he could not sit in one place for just three minutes. He kept saying, I cannot breathe. My heart is not working. And he was sweating a lot.." [100VE, #3]. One of the common symptoms of heart failure is "Shortness of breath while in rest or lying flat"[#4]. The heart-failure can be diagnosed by chest X-ray and blood tests. Some types of heart failure are curable, however, most may be found treatable but incurable [#4].
FAYSAL'S VISIT TO IHMS-GP1 (20/9/2016 -- 28/9/2016)
Certainly, Faysal's illness could not have developed within a short period of time. Therefore, Faysal must have been presenting IHMS with the same heart-failure symptoms long before September-2016. As such, times prior to Faysal's September visit of IHMS-GP1, it is possible that requests for further tests and treatments that made by IHMS have been rejected by DIBP/ABF. The consistent refusal by all IHMS-GPs to properly address Faysal's request on heart-failure symptoms indicates such DIBP order -- i.e. not to raise any RMM for Faysal -- that may have already been in place. This scenario is largely consistent with the DIBP Secretary's PE_003 Directive on June 2015.
The X-ray and blood tests instructed by IHMS-GP1 on 28/9/2016 may have confirmed the worsening condition of Faysal's heart failure. Experienced clinicians could have noticed irregular heart shapes or internal organs and the presence of fluid in the lung from the chest X-rays [#4]. The test results reflecting Faysal's condition would have been shared internally within IHMS and DIBP/ABF, without disclosing those facts to Faysal.
Whether the illness was treatable or incurable, the DIBP/ABF, IHMS and its GPs withholding such critical health information from Faysal have serious criminal implications including slavery laws. As noted above, the torture laws had already been violated when Faysal's requests for treatment had been denied by IHMS.
We will therefore proceed with our legal analysis based on two assumptions derived from anecdotal and other available evidence:
(i) the results of X-rays and a blood test undertaken by Faysal with 28-Sep-2016 instruction of IHMS-GP1 have been non-negative and the results are consistent with illness symptoms presented earlier;
(ii) the DIBP/ABF has instructed all IHMS Personnel to "keep silence" on Faysal's illness.
All IHMS Personnel, including ABF on Manus Island, are involved in withholding this critical, personal health information from Faysal. Consequent criminal implications heavily fell upon all IHMS-GPs who personally examined Faysal, especially from September to December 2016.
The Illness of Faysal Ahmed: Part - 1
Possible Cause of Death
[Broadcast: 27th Nov 2021 (3-min R)]
Friends, the cartoonist "Eaten Fish" had depicted the last days of Faysal in VSRA (psychiatrist isolation) compound. The Guardian publication featured this informative depiction on the death of Faysal as of 25/12/2016 [#14] . As an eye witness, Eaten Fish described further details on Faysal's illness symptoms :
-> Faysal had continuous, painful cough for 2 days since he arrived VSRA;
-> Faysal had been sweating alot; Faysal was heavy (due to fluid ?);
-> Faysal is heavy in breathing; wheezing sounds;
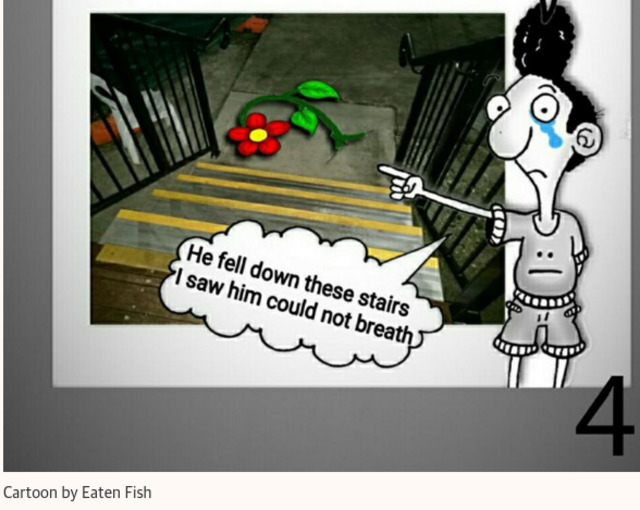
Eaten Fish (RUF-115) had witnessed Faysal Ishak Ahmed collapsing at psychiatric compound.
I have further consulted with two of the health resource websites [#11, #12], which indicated Faysal Ahmed may have died from "pulmonary edema". Pulmonary edema is a condition caused by excess fluid in the lungs. Cross-checking with symptoms described by Mayo Clinics here [#12], the matched items are:
=> Difficulty breathing with activity or when lying flat;
=> More shortness of breath than normal when you're physically active;
=> Wheezing;
=> Rapid weight gain;
=> Swelling in lower extremities;
=> New or worsening cough
Faysal, in his handwritten notes [#3], had reported all other symptoms above, except for the coughing. Faysal may be suffering from long-term cardiogenic pulmonary edema. The Mayo Clinics website [#12] further explains in detail how underlying heart failure may cause consequent pulmonary edema.
The Healthline website [#11] explained another similar illness, known as pleural effusion, where fluid build-up in the lungs, with the following symptoms:
=> breathing difficulties;
=> a dry cough;
=> shortness of breath;
=> chest pain and discomfort.
Faysal did report he had chest pains and heart problems. Both pulmonary edema and pleural effusion are resulted by a chronic heart failure.
For both pulmonary edema and pleural effusion, the patient must be immediately oxygenated before trying to address any underlying problems [#11, #12]. This means, for Faysal since September 2016, he should have been immediately hospitalised and brought under higher level care.
Friends, most of us are not medical doctors and are being humbled by the complexity of our bodies and the deeper knowledge of how all body parts are working in sync.
As for Faysal's illness, in the absence any proper official coronial report, I am satisfied for now that Faysal died either from pulmonary edema (40%) or pleural effusion (60%). The heart failure is to be primary underlying cause for built-up of excess fluid in Faysal's lungs.
The Illness of Faysal Ahmed: Part - 2
Underlying Cause of
Faysal Ahmed Illness
[Broadcast: 4th Feb 2023 (4-min R)]
Friends, as a layperson (I'm not a medical doctor), I have postulated the cause of Faysal illness in previous postings(2021) as [#15]:
Deriving from the evidence in hand, Faysal Ahmed may have been suffering from a long-term cardiogenic pulmonary edema. Faysal died either from pulmonary edema (40%) or pleural effusion (60%). The heart failure is to be the primary underlying cause for a build-up of excess fluid in Faysal's lungs.
My comment above was based on information from the final six months before the collapse of Faysal Ahmed on 22nd December 2016. I had given more weight on pleural effusion (60%) that that of pulmonary edema (40%), based on eyewitness evidence[#3] that Faysal was having distinctive cough when transferred to VSRA in Manus Island Detention Centre. Upon reviewing the primary information provided in the Guardian [#26], Faysal may have been suffering a far more serious illness -- cancerous growth or tumour for example -- in a much longer period. Walid (Sudanese refugee, Friend of Faysal) told:
He had severe stomach aches and the only medicine we received were pain relief tablets such as Panadol. He couldn’t sleep most nights because of the intensity of the pain.
That severe stomach pain, likely without a proper diagnosis and treatment, lasted for more than two years, of which that illness appeared to develop into "pleural effusion", with the common symptoms of chest pain, breathing difficulties and heart problems.
Of course, a layperson trying to postulate an already deceased person's illness can sound like making a "Wild Goose Chase"; But, not quite so in the view of Law. Such determination -- with the affidavit of expert medical opinion -- could become the "material evidence" that is inferred from the primary witnesses and available evidence.
PLEURAL EFFUSION, CAUSES, DIAGNOSIS & TREATMENT [#27]
Pleural effusion is a fairly common illness. In this academic medical resource guide, the underlying causes are identified and advised on diagnosis as [#27]:
Pleural effusion, the pathological accumulation of fluid in the pleural space, is very common...... Its causes vary widely, ranging from fairly harmless effusions accompanying viral pleuritis to .... due to congestive heart failure or cancer. Patients with a non-malignant pleural effusion have a one-year mortality in the range of 25% to 57% (1). The need to treat a pleural effusion and the therapeutic options for it are largely a function of its cause, which thus needs to be precisely determined in every case.
The most common symptom of pleural effusion is dyspnea [i.e. breathing difficulty]. The severity of dyspnea is only loosely correlated with the size of the effusion [Abnormal fluid collected in areas of the lung]. The pain symptoms were further explained:
The most common symptom arising from a pleural inflammatory response is pleuritic pain,..... The pain is usually felt in the region of the pathological abnormality, and it is often linked to the respiratory cycle. ..... Some patients describe a diffuse, painful sensation of pressure in the chest—particularly when ....... a primary malignant tumour, or pleural carcinomatosis. Pleural effusions in these situations are usually of the exudative type.
It could be that, in the case of Faysal, the two years of untreated tumour (or) cancerous growth, that caused severe stomach pain, had developed into pleural effusion in his final nine months of 2016. The beginning of Faysal's heart pain symptoms was described [#26]:
In April 2016, the responsibility for asylum seekers who received positive assessments as refugees was transferred to Oscar and Delta prisons, and Faysal was moved to Oscar......But entering Oscar prison was marked by two terrible incidents in Faysal’s life. First, he lost his mother ... in Sudan. And then Faysal began to experience severe heart problems.
The Sudanese refugee Walid described how the IHMS-GPs blatantly ignored Faysal's requests -- in the face of a patient who repeatedly collapsed -- to treat the illness [#26]:
Faysal became unconscious and collapsed over and over again but every time he visited the medical centre the doctor would tell him he was fine. On every occasion he returned empty handed and angry.
Friends, I shall update these findings on the section on the page of Faysal [#15]; And, perhaps if time permitting, the possibility of link-up with the results of chest X-ray and blood test that Faysal had undertaken on 28/9/2016.
-- Cheers, NetIPR.
The Illness of Faysal Ahmed: Part - 3
Timeline On
Faysal Ahmed Health Incident
[Broadcast: 17th Oct 2021 (7-min R)]
Friends, the following is the 'walk-through' detail evaluation on Faysal's health incident based on the primary and other reliable information. The consideration in this timeline will form the basis for allegations at ICC against the personnel and the organisations of IHMS, ABF and the Commonwealth. In compiling this timeline, the article by Sydney Morning Herald (30/12/2016 [#19]) has given the background on the emergence of these primary documents.
Another article that appeared in Independent Australia (15/5/2017 [#20]) explained the ways DIBP/ABF covered up in the aftermath of Faysal's death.
CONTENTS: THE EVIDENCE
- This collection of evidence consists of Faysal Ahmed's hand-written notes of requests for medical appointments to IHMS, together with the correspondence he had with IHMS and ABF. The collection also contains witness statements from Manus Island asylum-seekers including that of the Sudanese contingent. The date of these documents covered September to December 2016.
- The documents indicate that Faysal Ahmed had been suffering from chest pains, muscle tightness and breathing problems.
- Faysal Ahmed was examined by at least 3 different GPs who have stationed at Manus Island clinics at that time. In late September 2016, Faysal Ahmed had undergone chest X-rays and blood tests as per the instruction of one of the GPs.
- Faysal Ahmed had been told by the IHMS-GPs, Health Service Managers and ABF that "There is nothing wrong with him". The GPs refused to disclose to Faysal his medical test results, or the diagnosis as to why he had chest pains and breathing problems. At one stage, Faysal Ahmed had been told to see a psychiatrist for helps.
- In his last medical request form, Faysal Ahmed was asking a "reply in writing" whether IHMS could treat his illness. One of the IHMS-GPs reportedly told "verbally" to Faysal Ahmed that the IHMS cannot treat his chest pains and breathing problems.
- Faysal Ahmed collapsed on 22nd December 2016. He was airlifted to Brisbane hospital and died on 24th December.
- Till today (15/1/2022), and as of compiling these internet reports, the Coronial report for the cause of death of Faysal Ahmed has not been released to the public.
The content of primary evidence [#3] includes Faysal's handwritten notes, together with official correspondence between Faysal and the IHMS, ABF and Broadspectrum. The documents' timeline has covered the period from September 2016 to December 2016. Also emerged is that Faysal had been visiting IHMS Clinic for much earlier than September, where medical requests/complaints were being put forward in Arabic. Because no progress was made in him relieving the debilitating illness, Faysal had to seek help from a friend to translate the requests into English, which appears accelerated communications with the IHMS/ABF.

The requests (complaints) were marked by Feedback and Complaint (FC) form numbers. The following FC numbers were allocated from documents.
21/9/2016 FC6967a (BRS Feedback Complaint system)
6/10/2016 FC7061a
13/10/2016 FC7105a
22/10/2016 FC7184
The IHMS mentioned it had received 13 FC forms from Faysal [#20]. Therefore, other FC documents may have been in Arabic. The documents covered the tailing period of Sep-Dec 2016, before the eventual collapse of Faysal on 22/12/2016.
By looking at the pieces of evidence in hand, we may notice Faysal himself was fully aware that he has a serious illness. Faysal had made adequate initiatives in explaining his illness and he had systematically sought help from IHMS. This fact can be contrasted with two other Manus detainees, i.e. Hamid Shamshiripour and Salim Kyawning for example, who may have the difficulty in seeking help from IHMS concerning their illness, mainly due to delirium and lack of communication skills. The IHMS is therefore entirely responsible for failing to provide the requisite treatment plan for Faysal.
The seriousness of Faysal's illness had also been noted in the Sudanese Community's petition [100VE] and the narrative given by Manus Island asylum-seekers [101VE]. These two documents stand out as undisputed pieces of evidence.
FAYSAL'S MEDICAL TEST RESULTS
Two pieces of evidence [102PE] & [103PE] confirm Faysal's visit to IHMS-GP1 on 28/9/2016, where he was instructed to take chest X-ray and blood test. I presumed Faysal undertook those tests at Lorengau, a small local hospital located about 20min drive from the camp, where it has an X-ray facility and a pathology department. The existence of X-ray scan and blood test and the possible diagnosis of the illness of Faysal Ahmed had been given by ABF's CMO Dr. Brayley in a "closed session" of Parliamentary Inquiry on the 8/2/2017 [#21].
Exactly how IHMS Management and IHMS-GP1 had handled that non-negative test results for Faysal will have criminal consequences. Most likely, without informed consent from Faysal, the IHMS had internally arranged the expert file reading of results without physically examining Faysal. Remember, this is the observation of the likely "pattern" but not the "evidence". Whatever the IHMS internal procedures may have been, the evidence in hand is that the IHMS Management and IHMS-GP1 had "unilaterally" decided not to disclose the test results and deprive necessary treatment for Faysal. That conduct has criminal consequences on both torture and enslavement (see Sections VII and IX of [#9]).
On 6 October 2016, Faysal put forwards complaint about the IHMS GPs he'd been seeing [104PE]. Faysal stated he had collapsed recently from heart problem and had numb on his arm, hands and fingers; and there was no GP from IHMS had given treatment. The IHMS arranged for appointment with IHMS-GP2 on 12/10/2016.
On 14 October 2016, the Health Service Manager (HSM1) replied [106PE] to Faysal's complaint on 6th October. The letter addressed Faysal had been treated by the IHMS nurse and doctors; and stated there's no 'significant' weight loss they observed. The HSM1 advised Faysal to consult with mental health service for the sleeplessness.
On 23 October 2016, The ABF Operation Lead-Manus, Position Number 60031723, replied to Faysal [108PE]. The letter said if Faysal is confused with the treatment he received, the IHMS can provide with information.
The symptoms which Faysal had raised with IHMS GPs consistently had been the heart problems, chest pain, muscle tightness, the numb and swallowing of arms, hand and fingers. Faysal also clearly stated he had recently collapsed from heart problem [104PE]. The letters by ABF and HSM1 clearly showed 'deliberate indifference' to Faysal's 'serious medical needs'. These conduct clearly constitute torture. On the one hand, by placing apparently physically ill patient to psychiatric care, the ABF and IHMS/HSM1 were refusing to escalate Faysal's health care to a specialist treatment; preventing Faysal from receiving alternative health advise and care; coercing Faysal to be remained in detention camp. These conduct constitute torture with enslavement. These criminal charges will stand even in the absence of the knowledge of medical test results, about which Faysal had undertaken in September 2016.
We can postulate that in the last weeks of October 2016, Faysal had been physically weak and infirm as a result of the collapse and sleeplessness. On 22 October 2016, Faysal appeared to have put up a complaint again rebutting the health problems that he has had are not the result of mental illness [107PE]. The document is not on the official complaint form, but the scribble note that obviously attributing to the letter he received from HSM1. On that note, Faysal was clearly asking the IHMS-GP2 that his medical case be escalated to Senior Medical Officer.
In the Manus Island asylum-seeker community's narrative [100VE], Faysal used to get suffocated from cigarette smokes or perfumes, and asked Broadspectrum to provide him with a separate room. We can postulate that in December 2016, Faysal became very weak and lacking oxygen flows, and cannot sleep in a tent which he had shared with 25 other inmates. Faysal clearly needed to be hospitalised at that time. Whist a separate room wasn't available from Broadspectrum, Faysal appeared to have scaled his request down to having a new mattress, which might be more comfortable to sleep on. Broadspectrum replied that they're out of stock on mattresses [110PE]
On 15 December 2016, a week before he died, Faysal put up his complaint again through Broadspectrum [111PE]. Faysal notified if the IHMS GPs cannot treat his illness, to reply him in writing to that effect. He also suggested "don't wait treating me". That complaint was well publicised in Sydney Morning Herald and other reliable media outlets in December 2016. According to the investigative report in Independent Australia [#20], the Broadspectrum didn't pass down that complaint to IHMS, or having no FC number. The BRS failure to pass down a medical request by a patient also has criminal consequences.
In his final visit to IHMS-GP3, which likely to have taken place on 20-21 December 2016, Faysal had probably took along [111PE]. The IHMS-GP3 had told 'in verbal forms' the IHMS cannot treat Faysal's heart problems, muscle tightness and breathing difficulties. And also probably told Faysal not to come to IHMS again with those symptoms. With the state of Faysal's illness, IHMS-GP3 would have visually observed and noticed the physically deteriorating condition of Faysal, who at that time had been a very ill person that need immediate hospitalisation. The IHMS Management and GP3 refusal to treat Faysal constituted "authorities exhibiting deliberate indifference to serious medical needs" which translate to the crime of torture. Also by refusing to escalate Faysal's case to a higher level care with the sole purpose of containing the patient detainee's health crisis, within the purpose of remaining that detainee in the asylum camp; have constituted the crime of enslavement.
After the Sudanese Community submitted the petition to IHMS on 21 December 2016 [101VE], aftermath the authorities handling of Faysal's health situation would constitute torture and even, murder.
GOVERNMENT COVER UP VS. THE REACH OF TORTURE AND SLAVERY LAWS
In previous posting, we have discussed how the Commonwealth with detention groups have been withholding "material evidence" on Faysal's case. A material evidence is a piece of evidence which is important to prove a case. The evidence still being out of public viewing were summarised:
(i) the result of the X-ray and blood tests, which Faysal had undertaken by the instruction of IHMS-GP1 on 28/9/2016;
(ii) the diagnosis on those tests, which had already disclosed to the Senate Committee on 11/2/2017;
(iii) the Coronial post-mortem report on the death of Faysal, that said to have been completed after a year (i.e. 2017-2018).
By carefully evaluating the IHMS/ABF conduct regarding Faysal's illness, it can be seen that the IHMS GPs never officially recognised the main symptoms that were being put forward by Faysal: heart problem, chest pain, muscle tightness etc.. This is an orchestrated cover-up by IHMS management and GPs to prevent future legal liabilities. BRS/IHMS failure to comply with Faysal's request to give him in writing was one example [111PE]. This failure, in combination with the cover-up from Commonwealth/ABF has created a legally impenetrable shield, so to speak.
Of course, that would be the case if we are merely looking at the personal tort claims of medical negligence, murder or intent to kill. But, in torture and slavery laws within the contexts of the crime against humanity, we were not specifically looking at the evidence on the intent to kill and murder. We are looking at evidence on mistreatment, the confinement by coercion. That is where we can say, on Faysal's case, the legal cover-up shielded up by the Commonwealth and detention groups wouldn't even give a fig leaf's protection; the torture and slavery laws will strike it through.
Friends, I have uploaded Faysal Ahmed evidence summary file in the following URL:
http://www.aus4iccwitness.org/evidence/20161231_faysal-ahmed-evidence.pdf
Our next step is proper write-up with individual attribution, which we can send report to ICC.
CONSOLIDATED REFERENCES
[#1] https://parlinfo.aph.gov.au/parlInfo/search/display/display.w3p;db=COMMI...
[#2] https://casetext.com/case/monmouth-county-corr-inst-inmates-v-lanzaro
[#3] http://www.aus4iccwitness.org/evidence/20161231_faysal-ahmed-evidence.pdf
[#4] https://www.cedars-sinai.org/health-library/diseases-and-conditions/h/he...
[#5] https://www.cedars-sinai.org/blog/heart-attack-cardiac-arrest-and-heart-...
[#6] http://www.aus4iccwitness.org/node/94
[#7] http://www.aus4iccwitness.org/evidence/20171213_dibp-support-group-minut...
[#8] Australian Medical Association Code of Ethics
The AMA Code of Ethics 2004. Editorially Revised 2006. Revised 2016
https://ama.com.au/position-statement/code-ethics-2004-editorially-revis...
[#9] http://www.aus4iccwitness.org/node/92
[#10] http://www.aus4iccwitness.org/node/81
[#11] https://www.healthline.com/health/pulmonary-edema#vs-pleural-effusion
[#12] https://www.mayoclinic.org/diseases-conditions/pulmonary-edema/symptoms-...
[#13] https://casetext.com/case/maldonado-v-terhune
[#14] https://www.theguardian.com/australia-news/2016/dec/25/happy-bloody-chri...
[#15] http://www.aus4iccwitness.org/node/75
[#16] https://casetext.com/case/pace-v-fauver
[#17] https://johnmenadue.com/peter-young-why-health-professionals-in-immigrat...
[#18] https://en.wikipedia.org/wiki/Fritz_Klein
[#19] https://www.smh.com.au/politics/federal/i-need-you-guys-to-look-after-my...
[#20] https://independentaustralia.net/life/life-display/pre-empting-faysal-ah...
[#21] https://parlinfo.aph.gov.au/parlInfo/search/display/display.w3p;db=COMMI...
[#22] The of The Sutherland Shire vs Heyman (1985)
https://staging.hcourt.gov.au/assets/publications/judgments/1985/041--THE_COUNCIL_OF_THE_SHIRE_OF_SUTHERLAND_v._HEYMAN--(1985)_157_CLR_424.html
[#23] Breen vs Williams, HCA (1996)
http://www.aus4iccwitness.org/legal-resources/19960906_breen-v-williams-hca-judgment.pdf
[#24] LOWNS VS WOODS, NSW APPEAL CASE
http://www.aus4iccwitness.org/legal-resources/19960205_lowns-v-woods-nsw-appeal.pdf
[#25] Estelle v. Gamble, 429 U.S. 97 (1976)
https://casetext.com/case/estelle-v-gamble
THE RIGHT, THE WISE AND
THE IMBECILES OF OFFSHORE PROCESSING
( Broadcast 10 Oct 2021)
Friends, whilst I'm looking at Faysal's case and the behaviours of the medical doctors deployed by IHMS on Manus Island, my minds inevitably have drawn again into the actions taken by two great doctors: Dr Peter Young and Dr Nick Martin.

Dr Peter Young worked as the IHMS medical director for mental health since 2011, and resigned 2014. He testified before the Senate Inquiry in June 2015 that there have been DIBP intervention on the way IHMS doctors and psychiatrists reporting incidents [PE_006]. The reason and the way Dr Young stormed out of IHMS were probably outlined here [#1]. Most likely, he felt indignant about the IHMS imposed upon contractual conditions that are contrary to the ethical standards for medical practitioners. The doctor-patient relationship -- i.e. privacy, confidentiality and preserving the patient's rights -- were to have been governed by these ethical standards (Detailed discussion on Section VII [#2]). Non-observation on these time-honoured ethical standards, in the first instance, might violate patient's rights but wouldn't amount to breaking the laws (especially offshore). But, for Dr Young, as it would seems, any compromise on these ethical standards for medical practitioners has been unacceptable. As I can now reflect his action in 2014 and conclude that this has been awesome on rights.
Another great GP, Dr Nick Martin, have made his efforts going to refugee camps on Nauru. At the time he went to Republic of Nauru (2016), there's already enough controversy of that place; But, as formerly British Naval Officer, he was bold enough went into that island which he has historic family connection. Once he was on the job, he surely must have noticed unlawful medical practices. He had persevered on that crime scene for a year, helped refugees whichever ways he could [#3], then tell us and the world about the situation there [#3,#4]. Dr Martin, indeed is a brave and wise man, to my ways of thinking.
THE IHMS' IMBECILES
Going through detailed evidence on Faysal's case, the same thing cannot be said to those (three?) GPs deployed by IHMS on Manus Island. Their personal involvement on Faysal's case -- whichever ways being coerced by ABF and IHMS contracts -- leaving no rooms but the charge of torture with enslavement. Their conducts have shown that these GPs are the willing participants to the torture and enslavement scheme.
As for the IHMS, the ways it sets contracts out and instructing its GPs to administer medicine has fallen far short of "human ethical standards". The doctors administering medicine on asylum-seekers in a camp is different from the vet treating the "sheep and cows" on a paddock. Actions such as prohibiting doctors from disclosing medical information to patients; denying requisite treatment from patients; making unilateral decisions without informed consent by patients; these conducts will be construed in law as the practice of torture -- IHMS the principal perpetrator.
As for the ABF and Commonwealth, they are still withholding 'material evidence' on Faysal's case. These are:
(i) result of the X-ray and blood tests, which Faysal had undertaken by the instruction of IHMS-GP1 on 28/9/2016;
(ii) the diagnosis on those tests, which had already disclosed to the Senate Committee on 11/2/2017;
(iii) the Coronial post-mortem report on the death of Faysal, that said to have been completed after a year.
It remained to be seen that government withholding of these 'material evidence' would have in anyway being impeded our public investigation, or the application of torture and enslavement laws.
Friends, I invite you once again to visit ( http://www.aus4iccwitness.org/node/92 ), especially sections VII (Inalienable rights) and IX (Torture). There will be direct application of these laws onto Faysal's case.
-- Regards, NetIPR.
[#1] https://johnmenadue.com/peter-young-speaking-of-freedom-human-rights-and...
[#2] http://www.aus4iccwitness.org/node/92
[#3] https://meanjin.com.au/essays/the-nauru-diaries/
[#4] https://www.blueprintforfreespeech.net/en/prize/recipients/2019/dr-nick-...
APPEAL TO REFUGEE SUPPORTING COMMUNITY
( Broadcast 28 Aug 2019)
Friends, I really want you to revisit and re-examine the circumstances surrounding the death of Faysal Ahmed in December 2016. The reasons I'm inviting you to revisit this case has been not for you getting enraged; but to be able to methodically reflect upon the facts surrounding his death. As we all know, the thing on Manus and Nauru have been rolling on daily basis and, in a way to be sure from the LNP Government's point of views, the public should be "moving on" or "rolling along". But in the interest of justice, we must also be focusing on past misdeeds done by our government. The death of Faysal Ahmed is one such incident.
Available Public Information
There are some articles and other writings still being available on the Guardian [#1, #3] etc.. Reported then was that, in leads up to his death in December 2016, Faysal had visited IHMS clinic for more than 20 times in six months. Evan Faysal Ahmed's colleague detainees have had noticed the deterioration of his health. Why the IHMS doctor -- of any competence -- should not have noticed ? Why the IHMS doctor had not recommended him to further diagnosis, which obviously may required a medical evacuation from the camp.
The Guardian at that time, of course, would have put such questions to IHMS. But IHMS had avoided such scrutiny by saying “As this matter will be referred to the Queensland coroner, IHMS is not in a position to respond to your questions." The ABF's doctor John Brayley had also avoided the questions on the same ground [#3] at the Senate estimates. But, according to National Justice Project report [#2], no Coroner Inquest or judicial inquiry being on schedule. Clearly, on this case, the Government is avoiding scrutiny -- which is why we the activists need to have a serious look at that case.
The Existence of "Delay Committee"
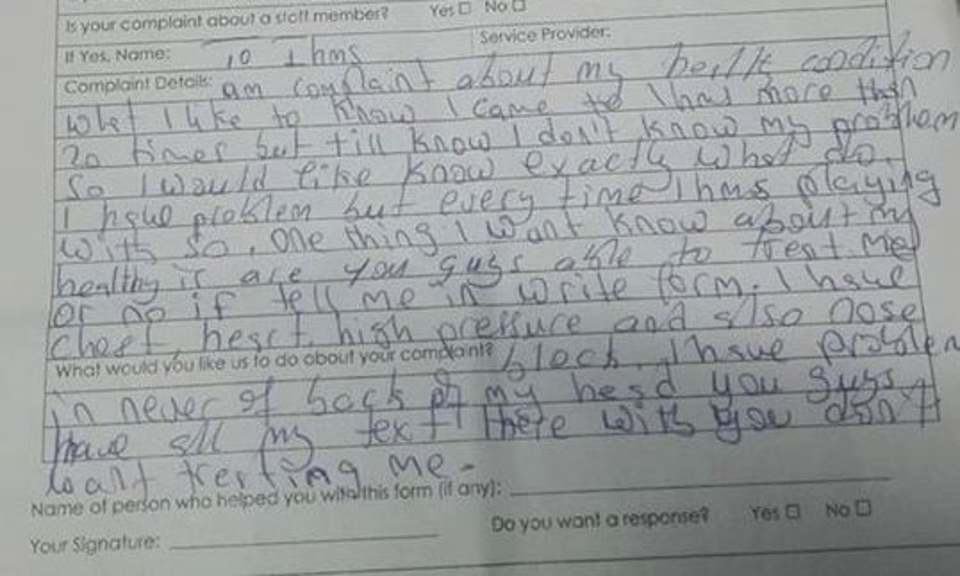
In lead up to enactment of Medevac legislation in 2018, there was an interesting ABC report which reveals the existence of "Transitory Persons Case Review Committee" [#4]. This is an internal working committee within ABF, which making final decisions on offshore medical transfers. Though, that was the first time we've heard of that Committee, my guess was that the same bureaucratic procedure would be in place as regards offshore medical evacuations since 2014. As such, that Committee is most likely to be responsible for the delays and, therefore, the deaths of asylum-seekers such as Faysal Ahmed.
Evidence of Committee: The Bromberg Judgment 2016
In fact, the trace of such Committee had already been exposed in the judgment delivered in May 2016 by Justice Bromberg at Federal Court [#5]. As we all know, in early 2016 a young refugee on Nauru fell pregnant after being raped, requested her pregnancy be terminated. The Department sent her to Port Moresby where the services & facilities may be inadequate and abortion was unlawful. The case of whether the Immigration Minister was negligent being determined by Justice Bromberg, at the behest of the High Court of Australia.
The importance of this judgment cannot be over stated (pdf downloads available here [#5]). The Judge had delivered on matters of the day in a comprehensive manners of which, the departmental process for medical transfer was exposed in details in Para. 112-157 of the report. Remember, these are the statements before a Judge and on a Court of Laws. They, therefore, stand as the proper evidence, as opposed to the normal news and media reports.
As it turns out, there was an "Offshore Health Division", which the First Assistant Secretary of (Mr Nockels) was in charge, which has been responsible for approvals of medical transfers. We can examine the behaviour of this "Offshore Health Division" for ourselves in above Paragraphs. With the given timelines of illness and death of Faysal Ahmed (September-December 2016), we can assume that the same fateful procedures were being in place.
As regards the behaviour of IHMS doctor on Manus, who may have "resisted" to treat Faysal Ahmed, or "refuse to escalate" him into proper medical transfer, would have the primary criminal responsibility. However, whether that IHMS doctor might have been following matters par the instructions of "Offshore Health Division", is as just still in our speculations of course.
QLD Coroner Report on Hamid Khazaei (July-2018)
The Coroners report for 2014 death of Hamid Khazaei had been handed down on July 2018 [#6]. I am looking for the same trace of the "Delay Committee", i.e. "Offshore Health Division". There are no obvious leads for the existence of the Delay Committee as such, and that is not to be surprised, of course! On the one hand, the Judge Terry Ryan had spelled out the scope of his inquest report as:
"23. An inquest is a fact finding exercise and not a process for allocating blame. The procedure and rules of evidence used in criminal and civil trials are not adopted. “In an inquest there are no parties, there is no indictment, there is no prosecution, there is no defence, there is no trial, simply an attempt to establish the facts. It is an inquisitorial process, a process of investigation quite unlike a trial.”
In that report too, there are "names of public servants" and "the events", which have caused the unnecessary delay of medical transfer of Hamid Khazaei. However, the link-up or chain-of-command were not being exposed on these delaying events, where the Judge Terry Ryan is not "required" to exhaust them any way. In some sense, the report had been "white washed" and that the information we're getting can be quite selective and not quite usable.
Striking Distance of ( 2 + 3 = 5 ) TRUTH ??
The feeling I get about this "Delay Committee" is that, there have already been enough information out there in the public domain about the characteristics of such Committee. In fact, throughout the years 2013-2019, there were several Senate Inquiries, investigative FOI publications and many other reports that were describing the Offshore Processing Process. It is a matter of properly examining these reports, in certain analytical ways, to reach to the truth. What I meant is, in any situation, we will get 2s and 3s of information, but we have to draw our own conclusions to get the desired result.
Remember, those criminals who were convicted of murder or paedophile do rarely admit to their guilt, at the court or in the public. Same too, those committed such heinous crimes as the Crime Against Humanity will rarely admit for their wrong doings. Even if we do wake up Joeseph Goebbels and Adolf Hitler from their graves, asking them to admit they've done wrong, will continued to deny and say they're working for the "national interests" and for the "love of father land". From the part of activists, what we need to do is to cut through lies and spins, use commonsense approach on finding the truth.
I ask our friends to keep researching the deaths of offshore asylum-seekers in the past several years; and share out any of your findings. Regards, NetIPR, (28-Aug-2019).
[#2] (No inquest in progress, according to NJP)
https://justice.org.au/inquest-begins-into-shocking-death-of-asylum-seeker/
[#3] https://www.theguardian.com/australia-news/2017/feb/10/manus-refugee-who...
Network for International Protection of Refugees
Est. 1998![]()
Objectives and Operational Procedures
Communications:
- 2023-Apr-18: State of Torture Law in Australia.
- 2022-Sep-18: to OTP-ICC, Submission of a preliminary finding and the Request for assertion of ICC jurisdiction .
- 2022-Feb-20: Detention Slavery, Submission to UN Special Rapporteur on Slavery.
- 2021-Sep-05: Follow-up letter to the Office of the Prosecutor of ICC.
LATEST UPDATE
Common law aspects of the doctor-patient contractual relationship in connection with the patient's natural (inalienable) rights in medical treatment. Examine Commonwealth Government's healthcare provision in offshore immigration detention based on the common law doctor-patient contract. Open public license 4.0 applied all content.

FEATURED
Collection of evidence and cases on detention slavery. Have chosen pieces of evidence that are reliable so that one can submit directly to the tribunal of fact. All evidence is taken from verifiable sources only. Two examples of enslavement with medevac delays on Faysal Ishak Ahmed and Samuel. Open public license 4.0 applied all content.

FEATURED
Australia's offshore processing scheme is interpreted within the context of enslavement of asylum-seekers. Starts with the applicability of Australian slavery laws at offshore settings, compare international and domestic slavery laws. Then, identify offshore medevac delay incidents as the indicators for slavery. Elucidate such delay incidents as violation of natural rights of human person, and that of Torture Laws and Slavery Laws.
